Proton radiotherapy is a form of ionizing radiation treatment using accelerated protons. The basic physical property of proton radiation is that they deliver most of their energy at the end of their path in the tissue, which is final and its depth is given by the initial energy of the protons. This leads to a dose distribution of radiation, which, compared to modern photon radiation therapy, places less burden on healthy tissues, especially in the middle and low dose range. Radiotherapy is an integral part of comprehensive cancer treatment. However, ionizing radiation treatment is always associated with a certain risk of side effects, which can manifest themselves months to decades after exposure. Thirty years after radiotherapy, the percentage of patients irradiated in childhood or juvenile age with very serious radiotherapy side effects (CTCAE grades 3 to 5) is between 30-50%. For these reasons, the field of radiation oncology seeks to develop technologies that will reduce the radiation exposure of healthy tissues while maintaining high-quality irradiation of the tumor site.
Physical Nature of Proton Radiotherapy
Photon radiotherapy irradiates the target volume from many directions so that the required dose is summed from these directions and, at the same time, the unwanted dose to healthy tissues is as low as possible. Particulate (in our case proton) radiotherapy allows to reach a sufficient dose to the target area while significantly minimizing the total irradiated volume of the surrounding structures. This is due to a different mechanism of interaction with the material between protons and photons. The photon beam is systematically weakened by the tissue, it releases most of its energy at the surface and passes through the whole body (Picture 1). In contrast, the proton beam conveys a small portion of the dose at the surface. The intensity of the dose increases in depth, reaches its maximum in the target area (this event is called Bragg peak) and the energy transfer no longer occurs behind it. It follows that proton irradiation is much more sparing in terms of the total radiation exposure of healthy tissues and equally effective in the area of the tumor site.
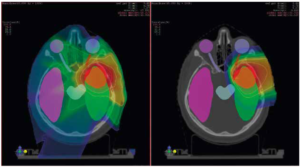
Picture 1 Comparison of irradiation using advanced photon technique IMRT (left) and proton beam irradiation (right). The target volume is marked in red. The dose distribution is shown by the color spectrum: the areas with the highest dose are shown in red and the dose is gradually reduced towards blue. If the given part of the anatomy is not covered by any color from the color spectrum (called colorwash), then there is no delivered dose. The picture shows a significantly larger volume of healthy tissue being irradiated during photon irradiation as opposed to proton irradiation.
Pencil beam scanning (PBS) technology
Modern proton centers use the PBS technology, as it is the most efficient way to deliver the required dose to the target volume while minimizing the doses to surrounding critical structures. With this method of irradiation, the target volume is divided into a grating, where an individually weighted proton beam is directed to each point of this grating. The result is a highly conformal irradiation of the target volume and, since no beam is directed outside this volume, also minimize doses to healthy tissues.
The PBS method has fundamentally changed the use and possibilities of proton radiotherapy. The tumor bed is divided into individual layers and these are divided into individual points. The beam is very thin (3-4 mm), its energy and depth of reach are gradually regulated, and it is directed to individual tumor points by means of scanning magnets located in the irradiator. The size of the irradiated area is not limited – it is in fact possible to irradiate very complex shapes. Adaptation to changes is relatively fast and neutron contamination is significantly less than for intensity modulated photon radiotherapy (IMRT) techniques with energies above 10 MeV. PBS was first used at the beginning of the millennium, but this technology did not become as popular until after 2010.
Radiobiological Bases
Another fact that must be taken into account when using particle therapy is the higher radiobiological efficiency of the proton beam compared to the reference photon beam. For the vast majority of protons, this efficiency is 1.1 times the efficiency of photon radiotherapy. This ratio is calculated when prescribing the dose. Therefore, it is possible to use protons in the same way as photons, in terms of doses and fractions in the above conversion. In recent years, it has become clear that at the very end of proton delivery, the radiobiological efficiency increases to 1.2-1.6 times the efficiency of photons. This is approximately the last 2 mm and, in most cases, this fact is of no clinical significance. However, in certain circumstances (for example, when irradiating brain tumors and using a single irradiation field), standard procedures need to be modified to take this into account.
Both methods are currently used for irradiation. The difference lays in the physical properties of individual types of radiation and thus different behavior in tissues. Photon radiation, the source of which is linear accelerators, shows a gradual dose drop in the tissue. This leads to greater “contamination” of the surrounding healthy tissues. When using protons, the dose drops steeply behind the radiation deposit in the target area. Compared to modern IMRT techniques, proton radiotherapy significantly reduces the burden on healthy tissues, especially in the area of medium and low doses. This means that a smaller volume of healthy tissue is irradiated. In some situations, the difference in dose distribution is clinically insignificant (for example in unilateral irradiation of the cervical nodes, irradiation of the entire cerebellum). In other situations, this difference is limiting to the use of photon RT (for example during irradiation of the thorax near the heart).
Proton radiotherapy can be used in a number of indications for radiotherapy. In the case of long life expectancies, proton therapy should be considered from a radiation protection perspective, despite the absence of randomized trials. Secondary malignancies are a problem in any type of radiotherapy and their induction is threshold-free – the requirement for radiation protection is to minimize doses to as low a level as is reasonably achievable. Randomized studies are a tool for evaluating new treatment methods. However here, more than a new method, it is a question of using the existing method (ionizing radiation treatment) but with a better tool. In addition, randomized data to confirm the predicted proton RT benefit in reducing late toxicity are not required in the NCCN guidelines. When deciding on the RT technique, it is recommended to consider the use of the most clinically sparing technique while maintaining sufficient coverage of the target volume. Patients after proton RT should then be monitored. Due to the physical characteristics of particle RT, which is more suitable for some patients indicated for irradiation, and to the improving availability of this technique, proton RT is most likely to partially replace photon radiotherapy in the future.
Purchase the book via the link below.
Purchase the book via the link below.

