
The main advantage of proton therapy is the significantly better dose distribution of the radiation dose to critical organs. Doses applied to the bladder and rectum are typically 25-50% compared to published doses for modern photon techniques. In the case of pelvic radiotherapy, the doses to the abdominal organs are 5-10% of the prescribed dose. The results of proton radiotherapy are better than recent published work for photon radiotherapy.
Particle radiotherapy in the treatment of prostate cancer achieves the best dose distributions of available radiotherapy techniques. Prospective non-randomized studies demonstrate its high efficacy and very low toxicity, and patients treated at PTC confirm these data.
Table 1: Comparison of effectiveness and toxicity of individual radiotherapeutic methods and the treatment of low-risk prostate cancer.
| Proton therapy | IMRT | Brachytherapy | |
| Efficacy (5-year disease-free survival) | 99% | 86-90% | 97% |
| Toxicity – genitourinary, Grade 2 and higher | <5% | 15-20% | 20-30% |
| Toxicity – gastrointestinary, Grade 2 and higher | 4% | 15-25% | 0-5% |
| Erectile dysfunction | 90% | 78% | 60% |
As evidenced by the data provided in the table, the undesirable effects after photon therapy are significantly higher than after proton radiotherapy.
Figure 1 and Table 2 are examples of an irradiation plan and dose distribution to individual organs. It is clear that a significantly lower or zero dose is applied to healthy tissue during proton radiotherapy.
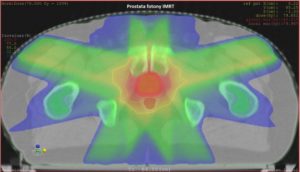
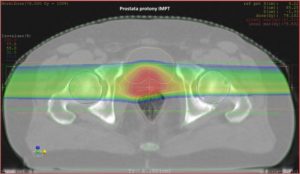
Figure 1: Example of a plan: photon IMRT vs. proton IMPT.
Table 2: Dose for each structure/organ.
| IMRT (photons) | IMPT (protons) | ||
| Target volume | Prostate | 78 Gy (100%) | 78 Gy (100%) |
| Organs at risk
|
Rectum Dmean | 40,2 Gy (51%) | 17,5 Gy (18,7%) |
| Bladder D(50%) | 9,5 Gy (12%) | 0,9 Gy (1%) |
Purchase the book via the link below.
Purchase the book via the link below.

